
5 Signs Your PCOS Diagnosis is Wrong
When I got off birth control after 13 years of taking it every single day, I stopped getting my period. One month passed, then two, six, and eventually a year, but I still didn’t get my period. It was devastating.
I did what anyone in my position would do: consult numerous doctors. They immediately diagnosed me with PCOS and suggested that I go back on birth control. But here’s the thing: other than my missing period, I had no other symptoms of PCOS. No weight gain, no thinning hair, no acne. On the outside, I was in perfect health.
Something was definitely wrong, but it wasn’t PCOS. After years of struggling, seeing numerous doctors and reading countless books to educate myself about my body and hormones, I finally found a functional doctor who was able to diagnose me correctly. I had something called “hypothalamic amenorrhea.”
Hypothalamic amenorrhea is a condition where you don’t get your period because your hypothalamus stops producing the hormones necessary to ovulate. I spent so many years chronically under-eating and over-exercising that my hypothalamus was focused on survival and stopped producing hormones necessary to reproduce. Plus, being on birth control further suppressed the production of those hormones which didn’t help.
But that’s a separate story. I’ve written about this part of my story in detail here.
Being misdiagnosed with PCOS sent me on a wild goose chase trying to find out what was wrong with my body while trying to fix it with the wrong solutions. It took a great toll on my physical and mental health. This article is an attempt to spare the unnecessary confusion and pain to others in the same position as me.
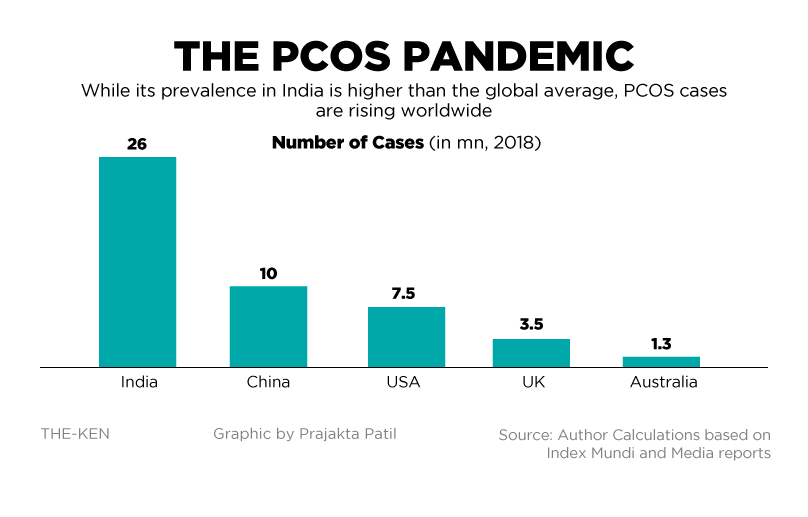
Polycystic Ovary Syndrome (PCOS) affects an estimated 8 to 13% of reproductive-aged women. Up to 70% of affected women remain undiagnosed worldwide. PCOS is the most common cause of anovulation and a leading cause of infertility. Since the rates of PCOS are exploding across the world (and especially in India), doctors are quick to assume that ANY hormonal imbalance is PCOS. (1)
No period? You have PCOS.
Irregular periods? PCOS.
Painful periods? PCOS.
This seems to be the general consensus but the reality is that this isn’t always true. There are other conditions that look like PCOS on the outside, but are actually something else entirely. If you’re someone who:
- Has gotten conflicting opinions from different doctors
- Has gotten a PCOS diagnosis recently but aren’t sure if it’s correct
- Has been trying to “cure your PCOS” but haven’t seen any positive changes
This article will finally help you understand what’s wrong. We’ll be diving into:
- What exactly is PCOS
- How is PCOS diagnosed and how standards have changed over time
- Why PCOS is likely to get misdiagnosed
- If not PCOS, what else could it be?
- How I knew I didn’t have PCOS
- How to make sure your diagnosis is correct
Let’s get started.
What Exactly is PCOS?
To understand what PCOS isn’t and to spot a potential misdiagnosis, we need to first understand what PCOS is. The best definition of PCOS I’ve come across is this:
“Polycystic ovary syndrome (PCOS) is one of the most common endocrine and metabolic disorders in premenopausal women. Heterogeneous by nature, PCOS is defined by a combination of signs and symptoms of androgen excess and ovarian dysfunction in the absence of other specific diagnoses.” (2)
“With PCOS, many small sacs of fluid develop along the outer edge of the ovary. These are called cysts. The small fluid-filled cysts contain immature eggs. These are called follicles. The follicles fail to regularly release eggs.” (3)
In simpler terms, PCOS (Polycystic Ovary Syndrome) is a condition that affects women’s hormones. If you have PCOS, your body makes more male hormones than usual, which can cause:
- Irregular periods: You might miss periods or have them less often.
- Excess hair and acne: You could have more hair on your face and body, and more pimples.
- Ovarian cysts: Your ovaries might have small cysts and not release eggs regularly, causing fertility issues.
Difference between PCOS and other diseases
You might wonder, why do so many women get misdiagnosed with PCOS?
The explanation to that starts with the name itself: Polycystic ovary syndrome (or disorder). Notice how PCOS is not a disease, but a syndrome.
What does that mean?
A disease is a specific pathological condition with a specific, defined cause such as an infection, genetic defect, or environmental factor. Diseases typically have a recognizable set of symptoms and a predictable progression. Basically, a disease is EASY to identify.
A few examples:
Diabetes can be diagnosed using the fasting blood glucose test, the A1C test, and/or the oral glucose tolerance test. Hypothyroidism can be detected using a TSH and free T3/T4 blood test that tells you if your thyroid is underactive. Iron deficiency anemia can be diagnosed using a comprehensive anemia panel that includes iron, ferritin, TIBC, iron saturation, b12, folate, reticulocyte count, and CBC. These conditions have measurable biomarkers that provide concrete answers.
In contrast, a syndrome is a collection of symptoms and signs that are often seen together but may not have a specific, identifiable cause. It is a set of medical conditions that occur at the same time and indicate a particular disorder, but it does not necessarily have a single underlying cause or pathology. PCOS is a great example of this. Other examples are IBS (Irritable Bowel Syndrome), Down Syndrome, etc.
With a syndrome, no two cases are the same, and every person will present a different combination of symptoms. There is no single test that can tell you whether you have PCOS or not. Instead, PCOS has certain “tell-tale” symptoms, like:
- Irregular or absent menstrual cycle
- Weight gain or difficulty losing weight
- Thinning hair or hair loss on the scalp
- Acne on the face, chest, and upper back
- Skin tags, which are small excess flaps of skin in the armpits or neck area
- Too much hair on the face, chin, or parts of the body where men usually have hair.
- Darkening of skin, particularly along neck creases, in the groin, and underneath breasts (4)
While these are great indicators for diagnosing PCOS, there’s a catch.
If a doctor sees any of these symptoms together, they’re quick to assume that it’s PCOS. But the doctors fail to recognize other common causes of the same symptoms.
How is PCOS Diagnosed?
Let’s get technical for a minute.
We’ve now established that since PCOS is a “syndrome” and not a “disease”, there is no conclusive test to diagnose PCOS. Instead, there are certain guidelines to determine whether someone has PCOS or not. These guidelines have changed drastically over the years.
In 1935, doctors S Irving Freiler Stein Sr. and Michael Leo Leventhal described PCOS after examining seven women who had the following symptoms:
- Hirsutism (excess hair growth)
- Obesity (being very overweight),
- Amenorrhea (missed periods), and
- Polycystic ovaries (enlarged ovaries with many small cysts)
Since then, various ways to diagnose PCOS have been suggested. In 1990, the National Institute of Child Health and Human Development defined PCOS as “having clinical (visible) and/or biochemical (blood test) signs of hyperandrogenism (excess male hormones) and oligo- or chronic anovulation (not ovulating regularly).”
If a doctor saw polycystic ovaries, it suggested PCOS but was not definitive. This view differed from that in the UK and Europe, where polycystic ovaries on ultrasound were seen as the key indicator of PCOS.
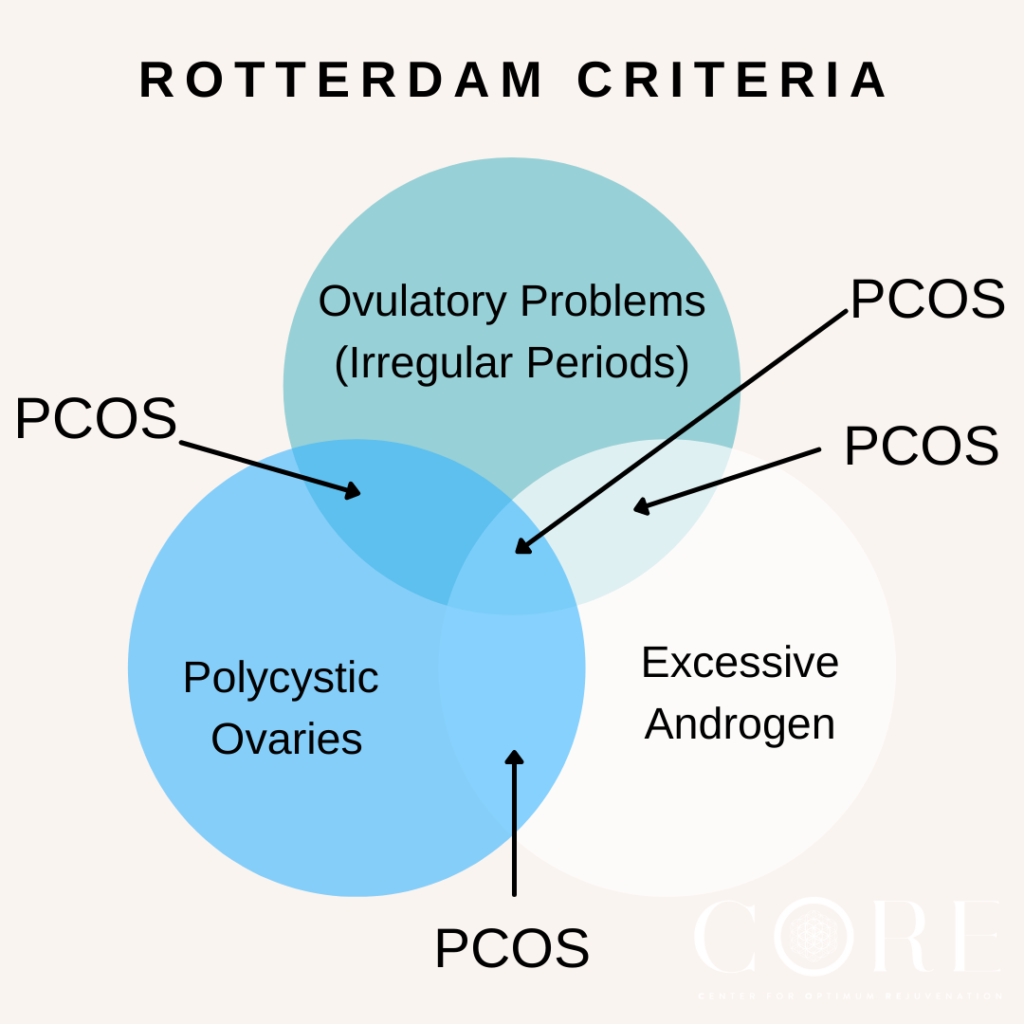
In 2003, 27 PCOS experts met in Rotterdam, Netherlands and created the “Rotterdam Criteria.” According to these criteria, a diagnosis of PCOS requires two out of three features:
- Irregular or missing ovulation
- Clinical and/or biochemical signs of hyperandrogenism, or
- Polycystic ovaries.
This broader definition increased the scope of PCOS compared to the 1990 NIH criteria, which required hyperandrogenism.
In 2006, the Androgen Excess Society (AES) emphasised hyperandrogenism for diagnosing PCOS while acknowledging the role of ovarian morphology. The AES criteria required hirsutism (excess facial hair) and/or biochemical hyperandrogenism (high levels of the sex hormone androgen), along with either oligo-anovulation or polycystic ovaries.
Finally in 2012, the NIH recommended using the “broader Rotterdam criteria“, identifying four sub-phenotypes:
- Androgen excess and ovulatory dysfunction (issues with ovulation)
- Androgen excess and PCOM (polycystic ovarian morphology)
- Ovulatory dysfunction and PCOM
- Androgen excess, ovulatory dysfunction, and PCOM
The Rotterdam criteria remains the most accepted and were reaffirmed in the 2018 International Evidence-Based Guideline for PCOS. (4) Your doctor should be using the Rotterdam criteria to diagnose you with PCOS.
Why is PCOS Overdiagnosed?
In the last section, we spoke about the changing diagnostic criteria for PCOS. While PCOS is the #1 cause of hormonal issues and infertility in women, there are many cases of mis or over-diagnosis. Let’s explore some reasons why:
- Broad diagnostic criteria: PCOS is associated with a wide range of symptoms that overlap with other conditions. This increases the likelihood of misdiagnosis. For example, symptoms like irregular menstrual cycles and acne can be caused by other hormonal imbalances (discussed later in the article).
- Lack of specific tests: There is no single definitive test for PCOS. This leaves to create our own explanation of the clinical symptoms and patient history. This approach is extremely subjective, and highly dependent on the doctor’s skill and experience.
- Heterogeneous nature: Since PCOS symptoms vary widely among individuals, some women might be diagnosed with PCOS based on minimal criteria, while others with similar symptoms might have a different underlying condition that is overlooked.
- Bias: Due to the rising rates of PCOS, doctors are quick to assume that any hormonal imbalance is PCOS. They do not factor in other conditions that have overlapping symptoms.
Here are 5 Signs You Have Been Misdiagnosed with PCOS
If you’ve been diagnosed with PCOS and think that your diagnosis is incorrect, here are 5 signs you should look out for:
- No elevated androgens: If your blood tests don’t show high levels of male hormones (androgens), your symptoms might be due to another condition. Hyperandrogenism is a key feature of PCOS, so normal androgen levels typically point to a different issue.
- Regular menstrual cycles: If your periods are regular, despite other symptoms like acne or excess hair growth, PCOS might not be the correct diagnosis. Women with PCOS often struggle to ovulate due to excess androgens, leading to irregular periods.
- Low body weight: If you have low body weight and missed periods, it could be functional hypothalamic amenorrhea, often caused by under-eating and excessive stress or exercise.
- Signs of other conditions: Conditions like hypothyroidism, Cushing’s syndrome, and adrenal hyperplasia can mimic PCOS. For example, weight gain, fatigue, and irregular periods can also be signs of hypothyroidism.
- Lack of ovarian cysts: If ultrasound scans show normal ovaries without multiple cysts, PCOS might not be the right diagnosis.
The biggest giveaway for me was that I did not have elevated androgens and did not have symptoms like acne and excessive facial hair. Moreover, I was underweight and exercising a lot, whereas people with PCOS tend to be overweight and sedentary.
If Not PCOS, What Could It Be?
We just discussed that PCOS could be misdiagnosed or overdiagnosed. The question remains: if you do not have PCOS, what is the cause of your symptoms like irregular periods, cystic acne, excessive weight gain or hirsutism?
Let’s explore some alternative diagnosis:
Alternate Diagnosis #1: Hypothyroidism
If you have irregular periods, weight gain, and fatigue, you could have hypothyroidism (an underactive thyroid gland). This means that your thyroid gland isn’t producing enough thyroid hormones which are crucial for regulating your metabolism, energy levels, and overall body functions. Hypothyroidism can be diagnosed by checking for high levels of thyroid-stimulating hormone (TSH) combined with low levels of free T4 and T3.
Alternate Diagnosis #2: Hyperprolactinemia
If you’re dealing with irregular menstrual cycles and elevated androgen levels, you could could have hyperprolactinemia, caused by a prolactin-secreting pituitary adenoma, a benign (non-cancerous) tumor in the pituitary gland that produces excess prolactin (a hormone responsible for stimulating milk production in women). Diagnosis typically involves blood tests to measure prolactin levels and imaging studies like MRI to confirm the existence of a tumor.
Alternate Diagnosis #3: Cushing’s Syndrome
Experiencing excess hair growth, irregular periods, and weight gain? You might be diagnosed with PCOS, but these symptoms can also be due to Cushing’s syndrome, which involves high cortisol levels. The diagnosis includes a physical exam, medical history, and specific tests to measure cortisol levels.
Alternate Diagnosis #4: Adrenal Hyperplasia
If you have hirsutism and menstrual irregularities, you could have non-classic congenital adrenal hyperplasia, a genetic disorder that affects steroid production. and leads to an imbalance in hormone levels.
You can diagnose it using blood tests that measure hormone levels, particularly 17-hydroxyprogesterone, and genetic testing to confirm the diagnosis.
Alternate Diagnosis #5: Hypothalamic Amenorrhea
If you’re missing periods and having low body fat, you could have hypothalamic amenorrhea, caused by stress and lifestyle factors. This was me for 16 years 🙋🏻♀️
After years of struggle, I was correctly diagnosed with Hypothalamic Amenorrhea.
Hypothalamic amenorrhea (HA) is a condition where the menstrual cycle stops because the brain stops making the hormones necessary to ovulate, often triggered by stress, significant weight loss, excessive exercise, under-eating, or a combination of these factors.
The diagnosis Involves ruling out other causes of missed periods, including PCOS, through blood tests, medical history, and physical examination.
This is what made it extremely difficult to diagnose in my case. Very few doctors understand hypothalamic amenorrhea and there is not much literature on it. It wasn’t until I saw a functional doctor who specialises in female hormones that I was finally able to figure out what I had. She immediately just knew based on my lab results and health history.
How to Make Sure You Get the Correct Diagnosis?
If you’re about to visit a doctor because you suspect you have PCOS (or any other hormonal imbalance), here’s a comprehensive list of tests your doctor needs to do:
- Check your complete medical history, including your previous lab work and any medical issues you have dealt with previously
- Consider all your symptoms, including any issues with your periods, male-pattern hair growth, any changes in your skin, unexplained weight gain, fatigue, bloating, poor digestion, bad sleep, etc
- Do a physical examination
- Do blood work to check your hormones, glucose, insulin, inflammation, and gut function
- Do a pelvic ultrasound to scan for ovarian cysts (5)
Further, all other endocrinopathies and hormone issues need to be ruled out first such as thyroid issues, prolactin related issues and congenital adrenal hyperplasia.
Make sure your doctor tests all the factors thoroughly and gives you a complete diagnosis.
And that’s a wrap. Do you know anyone who has PCOS or suspects they do? Share this article with them to make sure they have the correct information.


